Product information “Endometrial Carcinoma”
Clinical History
A 63-year old woman presented with a history of dull lower abdominal pain for 2 months and heavy persistent vaginal bleeding for 1 week. The menopause had occurred 13 years previously. Radical abdominal hysterectomy and bilateral salpingo-oophorectomy were commonly performed for the treatment of endometrial cancer following confirmation of endometrial carcinoma in biopsy.
Pathology
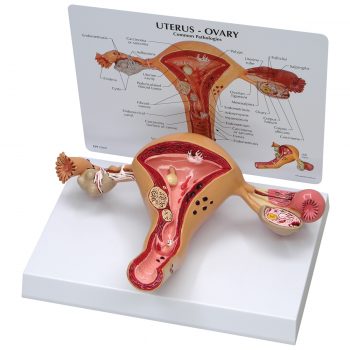
The specimen consists of uterus, fallopian tubes and ovaries. The endometrial cavity and endocervical canal have been opened on the anterior aspect. The endometrial lining is grossly abnormal especially on the right side and a brown polypoid tumour has invaded the myometrium and extends inferiorly into the cervical canal. Histologically this was a well-differentiated adenocarcinoma of the endometrium. The left ovary, which has been sectioned in the coronal plane, is enlarged and has several large follicular cysts/cavities.
Further Information
Endometrial carcinoma is the most common gynecological malignancy in developed countries and the second most common in developing countries after cervical cancer. There are two major types of endometrial carcinoma. Endometroid carcinoma account for almost 80% of endometrial carcinoma. They usually present early and so have a more favourable outcome. These tumours may arise from atypical endometrial hyperplasia. Common genetic abnormalities seen in endometrioid tumours are mutations in the PTEN, PIK3Ca and ARID1A genes. Serous carcinoma are a less common form of endometrial carcinoma. These tumours are associated with mutations in TP53 gene and carry a poorer prognosis. Endometrioid tumours tend to affect women aged 55 to 65 years. Risk factors for developing endometrioid endometrial cancer include obesity, impaired glucose tolerance, infertility, unopposed estrogen therapy (e.g. early menarche, late menopause or exogenous sources). Serous neoplasms affect older women aged 65 to 75 years with other risk factors for development include having a lower BMI and an atrophic uterus. Women with Hereditary Nonpolyposis Colorectal Cancer (Lynch Syndrome) have a significantly higher risk of developing endometrial cancer.
The most common symptom of endometrial cancer is abnormal vaginal bleeding. Most frequently it presents as post-menopausal bleeding, which often allows early presentation. Others may be asymptomatic or an incidental finding of an abnormal endometrium on abdominopelvic imaging. The main radiological sign of endometrial cancer is abnormally thickened endometrium on pelvic ultrasound or CT scan. Diagnosis is made on endometrial biopsy, endometrial curettage or hysterectomy. Treatment depends on the stage of the cancer and includes local radiotherapy, systemic chemotherapy and surgical hysterectomy +/- salpingo-oophorectomy.