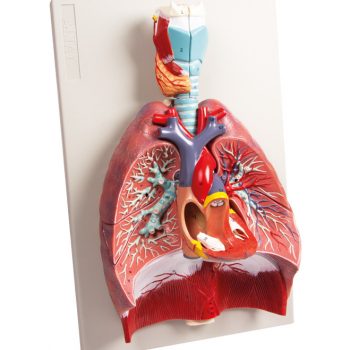
Product information “Lung—Cystic Fibrosis”
Clinical History
A 6-year old girl was admitted with a productive cough, dyspnoea and fevers. She became increasingly hypotensive and dies soon after admission. She had a previous history of recurrent pneumonia and meconium ileus. The clinical diagnosis was cystic fibrosis (mucoviscoidosis). Her sister died aged 3 from the same disease.
Pathology
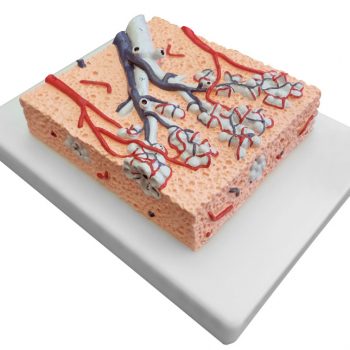
The lung parenchyma shows extensive changes mainly with a bronchial distribution. Many bronchi are dilated (bronchiectasis) and contain thick, yellowish, purulent material. These changes are most marked in the upper lobe, at the apex of which a small focus of ‘honeycomb’ change is also seen. Multiple abscesses are present, especially in the basal and central parts of the lower lobe. The base of the lower lobe is severely affected with fibrosis and consolidation being evident. There is very little normal lung tissue remaining. These pathological changes are characteristic but not pathognomonic of cystic fibrosis.
Further Information
Cystic fibrosis (CF) is an inherited disorder of chloride ion transport. Mutations in the cystic fibrosis conductance regulator (CFTR) gene on chromosome 7 cause defects in the chloride channel protein leading to dysfunction of the chloride channels. This causes increased water absorption in exocrine glands and epithelium of the respiratory, gastrointestinal and reproductive tracts. These dehydrated viscous secretions then obstruct these organ passage causing clinical features including: persistent pulmonary infection, pancreatic insufficiency, liver cirrhosis, intestinal obstruction, male infertility, and elevated sweat chloride levels. In the airway, CF patients have decreased chloride secretion and increased water reabsorption. This causes dehydrated mucous lining the airways leading to defective mucociliary action, mucous obstructing the airway, bronchiole dilatation (bronchiectasis) and secondary infection. Staphylococcus aureus, Haemophilus influenzae and Pseudomonas are the most common bacteria causing CF patients’ lower respiratory tract infections. Chronic bronchitis and bronchiectasis develops as a result. Pulmonary issues are the highest cause of mortality in CF patients. The average life expectancy is between 40-50 years of age in developed countries.
CF occurs in around 1 in 3000 live births. It is inherited in an autosomal recessive pattern. It is most common in fair-skinned populations: with 1 in 20 being a carrier of the gene. Symptoms can present in-utero or even up to adolescence, depending on the severity of the disease. It is now most commonly diagnosed with the neonatal screening test for immunoreactive trypsinogen (a pancreas enzyme precursor). If this screening test is positive, a formal diagnosis is made with a sweat test showing >60mmol/L of chloride.